Significant accomplishments
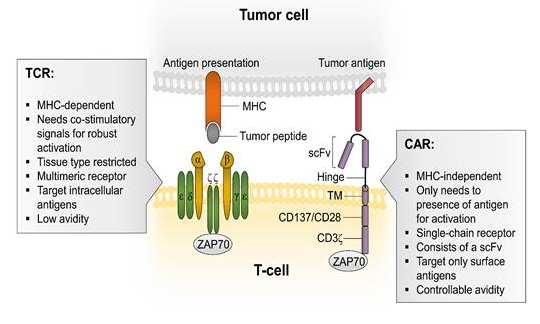
Figure 1. Differences between a TCR and a CAR (Poorebrahim et al, Crit Rev Clin Lab Sci. 2019).
© Poorebrahim et al, Crit Rev Clin Lab Sci. 2019
1. Engineered T cell receptor (TCR) and chimeric antigen receptor (CAR) T cells for immunotherapy of cervical and vulvar cancers caused by oncogenic human Papillomavirus.
Oncogenic human papillomaviruses (HPVs) are the main causative agents of cervical cancer, as well as anogenital and oropharynx carcinomas. Although prophylactic vaccines that prevent infection by the most prevalent oncogenic HPV types (specially HPV16 and 18) are available, people already infected by these viruses are at risk of developing HPV-related malignancies. The viral genes E6 and E7 are constitutively expressed in cervical intraepithelial neoplasia (CIN) of grades I to III and in invasive cervical cancer. Therefore, the E6 and E7 viral products represent ideal tumor antigens to be targeted. However, clinical studies with candidate therapeutic HPV vaccines have shown little success so far. Another arm of immunotherapy, checkpoint inhibitor blockade, has shown modest benefit in advanced or metastatic cervical cancer, restricted to the PDL-1 positive subgroup and no responses in vulvar cancer thus far.
Genetically engineered TCRs specific for E6 and E7 epitopes and chimeric antigen receptors (CARs) against surface tumor-associated antigens, when introduced in patient-derived peripheral T lymphocytes, can drive potent anti-tumor responses that, under favorable tumor microenvironment conditions, should result in an efficient immunotherapy of HPV-associated malignancies. The fundamental difference between TCRs and CARs resides in the fact that TCRs bind to molecules of the major histocompatibility complex presenting peptides from any (intra- or extracellular, endogenous or exogenous) protein, CARs are receptors targeting surface antigens expressed preferentially on cancer cells (figure 1).
The overall aim of this project is the development of engineered TCR and/or CAR T cell immunotherapies targeting tumor cells in HPV-related malignancies on the basis of a diagnostic/prognostic immunologic platform that defines the tumor macro- and microenvironments.
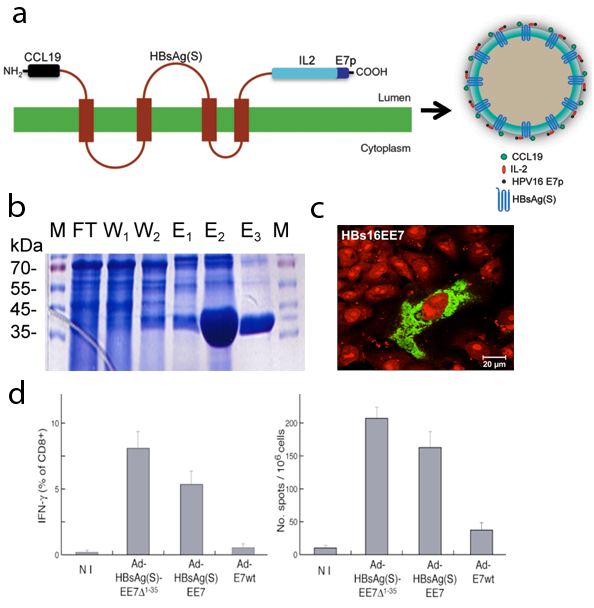
Figure 2. Design, expression and characterization of vaccines based on virus-like particles (VLPs). (a) Schematic representation of HBsAg(S) bearing CCL19, IL-2 and an HPV-16 E7 peptide and its assembly in VLPs. (b) Coomassie blue staining of flow-through (FT), wash (W) and elution (E) fractions from an ion metal affinity chromatography (IMAC) of a His-tagged recombinant HBsAg-E7 protein expressed in the yeast P. pastoris. (c) Confocal microscopy of a transfected Vero cell expressing HBsAg-E7 (in green), the nuclei are stained with propidium iodide (red). (d) Specific anti-E7 T cell responses in mice immunized with Ad-HBsAg-EE7 (synthetic, codon optimized gene), Ad-HBsAg-EE7(D1-35), or Ad-HBsAg-E7 (wild-type gene).
© dkfz.de
2. Design, construction and characterization of vaccines based on virus-like particles (VLPs) carrying specific tumor antigens. We have engineered chimeric hepatitis B surface antigen (HBsAg) VLPs, which harbor human Papillomavirus (HPV) T cell epitopes and cytokine domains while still preserve their capability to self-assemble into VLPs.
The oncogenic HPV types 16 and 18 are associated with precancerous lesions in the uterine cervix (cervical intraepithelial neoplasia, CIN) that eventually progress to cervical cancer. They are also associated with anogenital and oropharingeal cancers.
Individuals infected by these viruses cannot take advantage of the prophylactic HPV vaccines and are at risk of developing HPV-related cancer. However, these patients could benefit from vaccines that activate T cell effector cells against HPV-infected tumor cells.
We have shown that codon optimization of the viral genes facilitates the production of protein vaccines (Cid-Arregui and zur Hausen, Modified HPV E6 and E7 genes and proteins useful for vaccination, US Patent 7,201,908 B2, 2007). Yet, overexpression of E7 in human cells results in significant cytotoxicity. Immunization of HLA-A2 transgenic mice either with plasmids or recombinant adenoviruses engineered to express HPV-16 E7-HBsAg chimeric particles evoke strong B and T cell responses (figure 2). Addition of the chemokine CCL19 and interleukin 2 (IL-2) to the HBsAg-E7 particles significantly enhanced the anti-E7 T cell responses in the absence of adjuvant (Cid-Arregui, A. and zur Hausen, Fusion polypeptides and their use for prevention and treatment of cancer, patent EP2335730 A1, 2011).
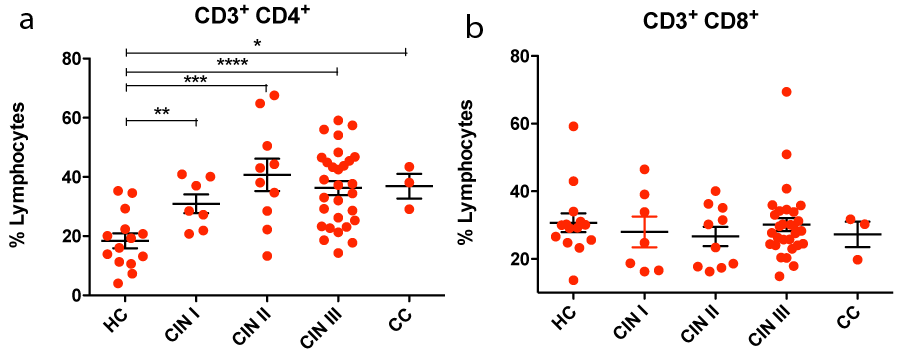
Figure 3. Frequency of circulating CD3+/CD4+ (a) and CD3+/CD8+ (b) double positive cells in healthy controls (HC), in cervical intraepithelial neoplasia (CIN grades I, II and III) and in cervical cancer (CC) patients. The graph in (a) shows a significant increase of CD3+/CD4+ cells in CIN and CC patients.
© dkfz.de
3. Explore diagnostic and prognostic markers for CIN and cervical cancer. Progression from CIN to cervical cancer is associated with altered circulating levels of cytokines. We have designed a prospective cohort study to determine the levels in serum of a large number of cytokines. A cohort of patients with cervical pathology (CIN I, CIN II, CIN III and invasive squamous cell carcinoma) as well as healthy donors has been enrolled for this study at the National Center for Tumor Diseases and the Gynecology Department of the University Hospital in Heidelberg in collaboration with Prof Dr. Frederik Marmé. Measurement of the serum concentration of cytokines is being performed using a bead-based sandwich immunoassay, the LEGENDplex Human Th Cytokine and Human Inflammation Panels (BioLegend), which include the following cytokines: IL-2, IL-4, IL-5, IL-9, IL-13, IL-21 and IL-22; and IL-1b, IL-6, IL-8, IL-10, IL-12p70, IL-17A, IL-18, IL-23, IFN-g, TNF-a and MCP-1, respectively. Preliminary results have shown that progression from low to high grade CIN and cervical cancer is associated with altered levels of Th1/Th2 and proinflammatory cytokines, indicating the potential balance that cytokines can exert in the immunologic control of cervical cancer and that circulating levels of some of the above cytokines could be useful in identifying women at higher risk of developing cervical invasive cancer when altered levels are detected at the CIN I/CIN II stages. In addition, we analyze the frequencies and phenotypes of CD4+ and CD8+ cells in the blood of CIN and cervical cancer patients compared with healthy donors (Figure 3). Based on immunosequencing, we have started a systematic study of the immune receptor (TCR) profiles of peripheral blood T cells isolated from CIN and cervical cancer patients, and healthy donors. This approach should reveal the numbers and diversity of T cell clonotypes in the CIN and cervical cancer-infiltrating lymphocytes, which will be compared with the circulating TCR clonal expansion profiles. Immunoprofiling will reveal differentially expanded clones throughout the different stages of the disease, providing the basis for new immune diagnostic and prognostic tools.
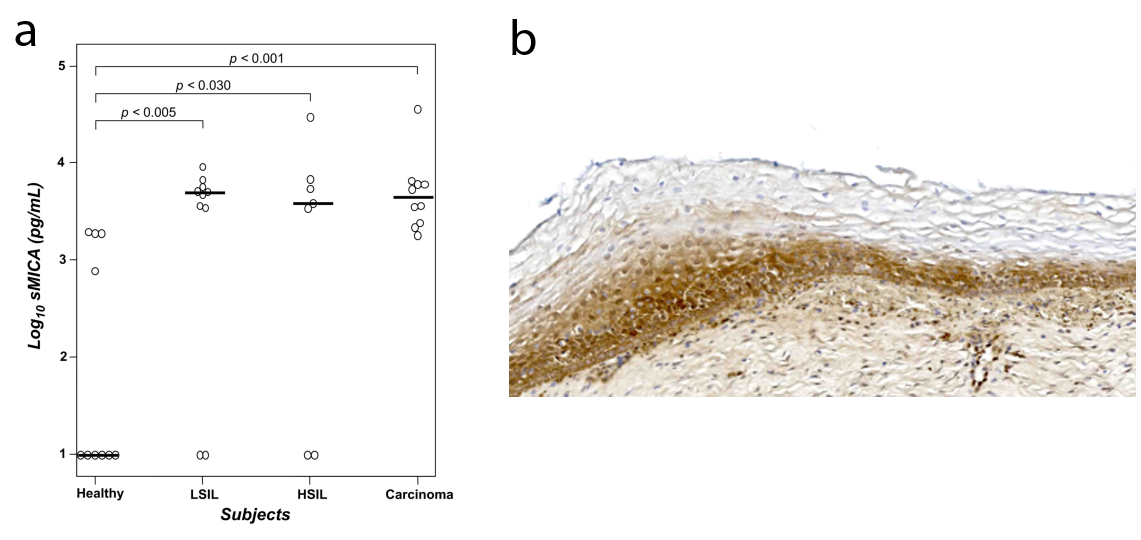
Figure 4. (a) Increased serum levels of soluble MICA in the serum of CIN and cervical cancer patients compared to healthy donors; and (b) expression of B7-H6, a ligand for the NK cell activating receptor NKp30, in CIN I.
© dkfz.de
4. Investigate innate immune responses in cervical cancer patients. The innate immune response is considered to be the first line of defense at mucosal surfaces. NK cells represent an important arm of the innate immune system specialized in killing virus-infected and tumor cells through the NKG2D activating receptor. NKG2D can promote the lysis of target cells by binding to ligands encoded by the MHC class I chain-related (MIC) genes. The MIC family includes MICA, MICB and ULBP1-6. NKG2D ligands are overexpressed in a number of epithelial tumors. NKG2D engagement by its ligands induces proliferation, survival, and, cytotoxic activity in NK cells. However, the shedding of MICA from the cell surface has been demonstrated in a variety of malignant epithelial tumors, including cervical cancer. Shedding leads to accumulation of soluble MICA (sMICA) in serum leading to NKG2D down-modulation by facilitating its internalization and lysosomal degradation. This has been proposed to be a mechanism used by cancer cells to evade NK-mediated tumor surveillance. We have shown an increase of soluble MICA (sMICA) levels in serum during progression of HPV-induced premalignant lesions to cervical cancer (figure 4a). Thus, shedding of sMICA might be a critical immune evasion event in the natural history of cervical cancer. Moreover, we also investigate the expression of B7H6, a ligand for the NK cell activating receptor NKp30, in CIN and cervical cancer tissues (figure 4b).
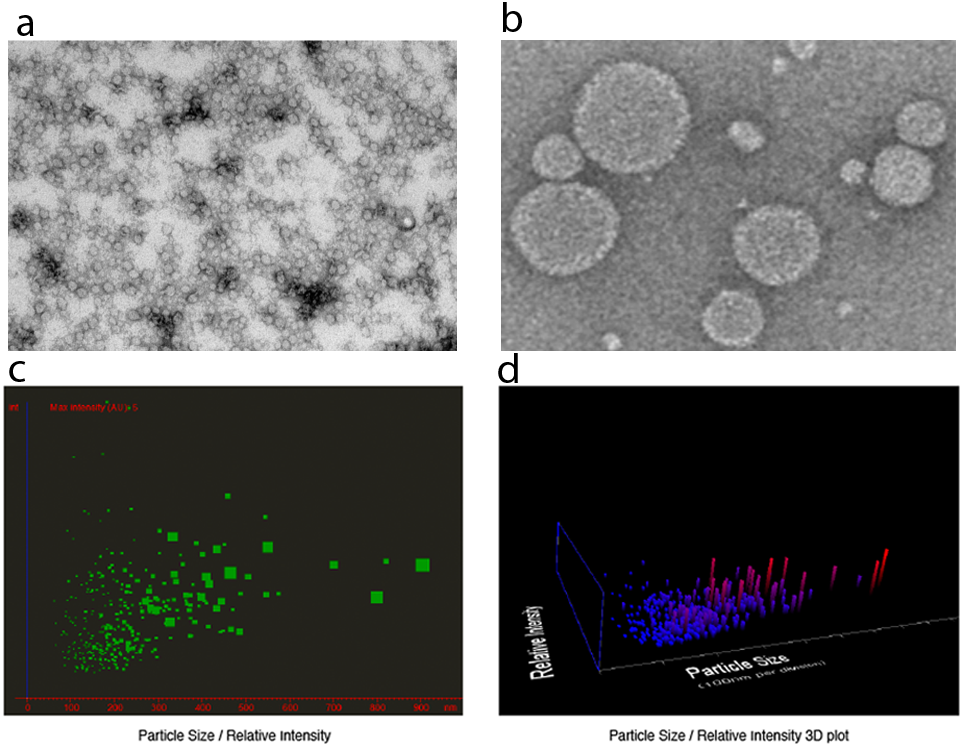
Figure 5. Transmission electron microscopy of negatively stained (a) hollow nanoparticles derived from an HBsAg deletion mutant as carriers for chemotherapeutic drugs; and (b) liposomes loaded with doxorubicin. (c, d) Particle size distribution profile of liposomes analyzed under scatter mode using the Nanosight system.
© dkfz.de
5. Develop liposomal/VLP-based drug delivery systems. Chemotherapeutic agents are far from ideal because they have been selected for their activity against proliferating cells, and they do not discriminate between tumor cells and normal cells undergoing rapid division. In addition, many potentially useful chemotherapeutic agents show poor water solubility and hence are difficult to deliver through traditional methods. Therefore, attempts are being made to develop delivery systems to improve both targeting and efficacy of drug delivery. However, there are considerable problems with many of the current in vivo delivery systems for therapeutic drugs. We have developed hollow nanoparticles in the form of membrane-enclosed vesicles comprising a truncated form of an HBsAg(S) protein lacking one or two of its amino-terminal transmembrane domains and a targeting domain, such as an integrin binding peptide or a pre-S1 binding domain (Cid-Arregui, Hollow nanoparticles and uses therefor, patent EP2262489 A2, US20110052496 A1, 2011). These particles (figure 5) can be loaded with chemotherapeutic agents to be delivered to tumor cells. In addition, we are approaching the targeting of liposomal nanoparticles to tumor cells and antigen presenting cells using various types of molecules, such as peptides, aptamers and single chain antibodies.